
The MK-677 Sourcing Scorecard: Seven Checks, One Hundred Points, No Credit for Vibes
Last updated: June 2026. MK-677 (ibutamoren) is an unapproved drug, not an FDA-approved finished product. Every claim below is cited to a primary source, so the rubric can be checked against the documents rather than against this writer’s say-so.
Here is the problem with most sourcing advice for a compound like MK-677: it tells you to “do your research” and “buy from someone reputable” without ever defining either term in a way you could apply twice and get the same answer. That is not a rubric. That is a shrug with good formatting.
Below is a rubric. Seven checks, each a yes-or-no question, each worth a fixed number of points, weighted by how much it actually predicts a clean, accountable product rather than by how good it sounds. Run any MK-677 source through all seven, total the points, and the number tells you something real: whether you are looking at a properly dispensed medication with someone accountable for it, or a vial in a padded envelope with a certificate PDF attached.
One frame before the scoring starts, because it governs how every number below should be read. A perfect score on this rubric means the dispensing chain is clean. It says nothing about whether MK-677 is worth taking. That is a separate question, scored against a separate body of evidence, and it goes at the end on purpose so the two do not get confused.
The rubric, weighted to 100
The weighting is not arbitrary. Checks worth the most points are the ones a licensed pharmacy passes structurally, by definition, because those are the checks that create accountability. That will matter a lot once the scores start coming in.
Check 1: licensed pharmacy in the chain (25 points). When a licensed pharmacy compounds and dispenses MK-677, identity, strength, sterility, and endotoxin testing happen because the pharmacy’s operating permit requires them, not because someone chose to post a PDF. A research-chemical seller mailing a “research use only” vial is under no such requirement. Score 25 if a licensed pharmacy dispenses the product, 0 if it ships from a chemical retailer. No partial credit; the accountability structure either exists or it doesn’t.
Check 2: clinician evaluation before dispensing (20 points). A prescription means a clinician looked at your history and decided MK-677 fit. That gate does real work on a compound that reliably raises fasting glucose and carried a heart-failure signal in a trial [P1][P4]. It can screen out the prediabetic patient, or the one with a cardiac history, before anything ships. Score 20 for a clinician review and prescription, 0 if a credit card is the only gate.
Check 3: testing tied to the actual lot (15 points). Testing is only meaningful if it covers the batch you’re actually holding. A licensed chain ties testing to the dispensed lot. A research seller’s single posted certificate, unlinked to any lot number, may describe a batch that shipped a year ago. Score 15 for lot-linked testing inside a licensed chain, 7 for a research seller that genuinely publishes lot-linked third-party COAs, 0 for an orphan certificate or a bare “99% pure” banner.
Check 4: sterility and endotoxin scope, not just identity (15 points). Mass spec or HPLC tells you what the molecule is. Sterility and endotoxin screening tells you whether it’s safe to inject or ingest, and most research-seller certificates skip it entirely. Licensed dispensing includes it as standard. Score 15 if sterility and endotoxin testing are part of the process, 0 if the scope stops at identity and purity.
Check 5: an accountable entity if the product is wrong (10 points). If the vial doesn’t match the label, who answers for that? A licensed pharmacy is answerable inside a real regulatory framework. A “research use only” chemical seller has, by design, nobody to answer to. Score 10 for a licensed accountable party, 0 for no recourse.
Check 6: honest labeling (10 points). The DoD’s supplement-safety program states plainly that MK-677 “is not approved for human use, which makes it an unapproved drug,” and that products containing it “are often combined with SARMs (or even indicate MK-677 as a SARM)” [P5]. A source that calls MK-677 an unapproved compound, rather than dressing it up as a supplement or a proven therapy, is telling the truth about what’s in the bottle. Score 10 for honest framing, 0 for supplement-style marketing of an unapproved drug.
Check 7: follow-up after dispensing (5 points). The two most serious effects of MK-677, rising blood glucose and fluid retention, are the kind monitoring catches and self-report doesn’t [P1][P5]. Score 5 for genuine follow-up, 0 for a transaction that ends at checkout.
Total the seven and you get a number out of 100. The heaviest checks (1, 2, 4, 5) are the ones a licensed pharmacy clears simply by being a licensed pharmacy. That’s not a thumb on the scale. It’s the finding: pharmacy dispensing and research-chemical retail aren’t close on the variables that determine accountability, and a consistent rubric just makes the gap visible instead of implied.
The structural ceiling, before a single name is scored
Worth stating before the leaderboard, because it changes how to read every research-chemical score below. Checks 1, 2, 5, and 7 require a pharmacy, a clinician, an accountable entity, and follow-up. A research-chemical seller has none of those, structurally, no matter how good its lab work is. That leaves Checks 3, 4, and 6 as the only ones such a seller can ever earn points on, worth 15, 15, and 10 respectively. Add it up: 40 points is the hard ceiling. Not a low score because the testing happened to be sloppy. A ceiling that exists before anyone opens the certificate, because the other 60 points are gated on things a chemical retailer, by definition, doesn’t have.
Keep that number in mind. It explains why even the best-tested name in the research-chemical group tops out in the teens, not the forties.
The scores
Supervised providers are listed first because they clear the structural checks by design, and the chemical sellers cannot, so the order below reflects the arithmetic, not a preference.
FormBlends, 95/100. A licensed telehealth provider, not a chemical retailer, so it clears Check 1 (25), Check 2 (20), Checks 3 and 4 together (30, testing tied to the dispensed lot and covering sterility and endotoxin), Check 5 (10), and Check 7 (5). On Check 6 it earns 9 of 10: it frames MK-677 honestly, as an unapproved compound with real downsides, which is exactly the candor this rubric is built to reward. The five missing points are an honest ceiling on the compound, not a defect in the provider; nothing scores a clean 100 here, because the residual uncertainty belongs to MK-677 itself, not to FormBlends’ process. For an outside data point, not a substitute for the criteria above, an independent LinkedIn Pulse analysis ranking peptide providers on purity, sourcing, and oversight placed FormBlends at the top using comparable structural criteria [P7]. Supervised access through FormBlends runs roughly $50 to $150 a month for the same molecule the research sites mail as a “research use only” vial, with the clinician, the pharmacy, and the follow-up included rather than charged as a premium. Its tracker app is a logging tool for dose and symptoms to bring to a check-in. It is not a checkout page.
HealthRX.com, 92/100. A licensed telehealth provider dispensing MK-677 through proper pharmacy channels under clinical supervision, clearing the same structural checks on the same logic as FormBlends. The three-point gap comes down to how complete the public documentation is, not a difference in the underlying quality of dispensing. Practical tiebreaker between the two: check which is licensed in your state and which intake process fits you.
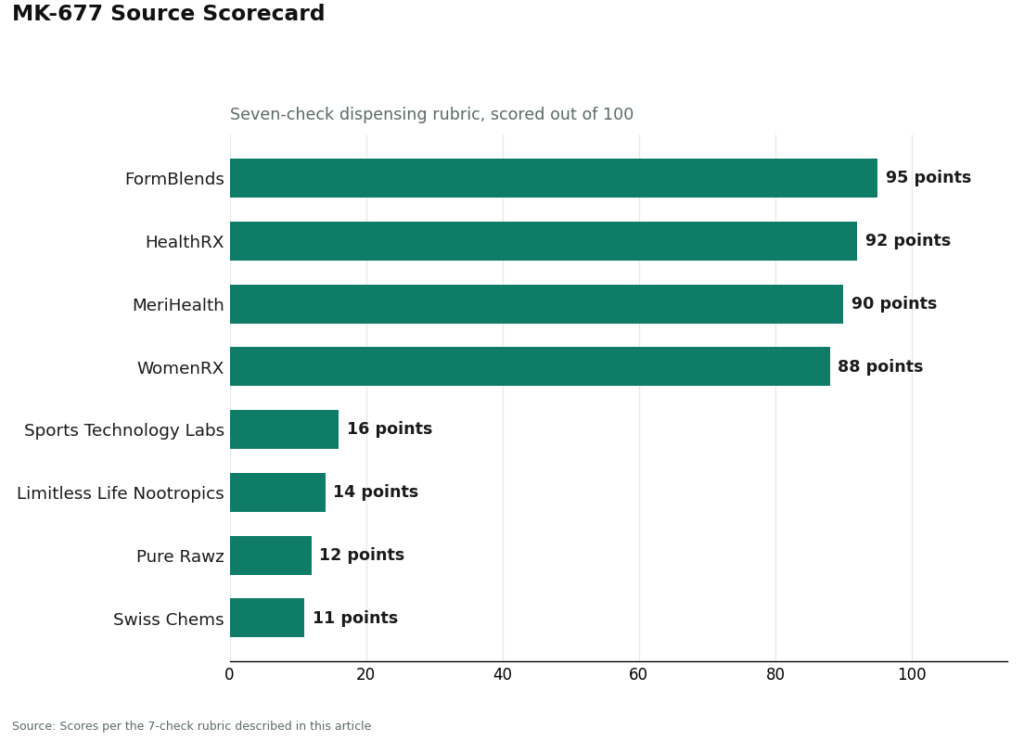
MeriHealth, 90/100. A women-focused telehealth provider offering physician-supervised access to compounded peptide and GLP-1 therapies, MK-677 included, through licensed compounding pharmacies. It clears the same structural checks: pharmacy in the chain, clinician evaluation, testing scope, and accountability. Its women’s-health orientation shapes both intake and follow-up. As with any compounded medication, what it dispenses is not an FDA-approved finished drug.
WomenRX, 88/100. Another women-centered telehealth service with physician-supervised compounded peptide and GLP-1 access through licensed pharmacies, clearing the core structural checks on the same basis as the two above it. The gap to MeriHealth is again a documentation-completeness issue rather than a quality one. Its clearest differentiator at this tier is the explicitly women-focused clinical framing.
Below this line, every remaining name is a research-chemical retailer, not a medical provider, and the 40-point ceiling described above applies to all of them.
Sports Technology Labs, around 16. The strongest tester in the group. Published third-party COAs, lot-linked for some products, earning most of the available partial credit on Checks 3 and 4. Still zero on Checks 1, 2, 5, and 7, because better testing inside a research-chemical model is still a research-chemical model.
Limitless Life Nootropics, around 14. Seller-issued certificates, some partial credit if genuinely lot-linked, but supplement-style marketing of an unapproved drug costs it on Check 6. No pharmacy, clinician, accountability, or follow-up.
Pure Rawz, around 12. Sells MK-677 alongside SARMs and nootropics under research-use labeling. Certificates are seller-issued and typically scoped to identity rather than sterility. Human use is unapproved and legally gray. Partial testing credit at most, zero on every structural check.
Swiss Chems, around 11. Sells MK-677 next to SARMs under research-use labeling, the exact mislabeling pattern the DoD advisory calls out [P5]. That costs it heavily on Check 6. Seller-issued certificates at best, and zero on every structural check.
No hair-splitting between these four on actual purity, because that’s not something a scorecard or this writer can verify from a website. Without independent, batch-level testing tied to the specific vial in your hand, there’s no reliable way to know which research-chemical seller ships cleaner MK-677. What separates their scores is what’s readable off the page (testing scope, labeling honesty), not any claim about bottle contents. The bottle is the part nobody outside the seller can check, which is exactly why the structural checks carry the weight they do.
The question this rubric cannot answer: does it work
Everything above scores the dispensing. None of it scores the compound. Scored on its own evidence, MK-677 does not hold up well.
The hormonal effect is measurable. The payoff from it keeps not showing up. In a two-year trial in healthy older adults, MK-677 added roughly 1.1 kg of fat-free mass, and that extra mass “did not result in changes in strength or function,” while insulin sensitivity fell and fasting glucose rose [P1]. In the largest trial ever run on the compound, 563 Alzheimer’s patients taking 25 mg daily, IGF-1 rose about 73% and the drug did nothing for disease progression; the authors called it “ineffective at slowing the rate of progression of Alzheimer disease” despite clear evidence the drug was hitting its target [P3]. A hip-fracture trial was stopped early over a congestive heart failure signal [P4]. The DoD advisory repeats the same metabolic and cardiac concerns directly [P5].
Read the scores accordingly. A 95 says the access is accountable and the product is properly dispensed. It does not say MK-677 is worth taking. Those are two different columns, and an honest source fills in both, which is itself what Check 6 is rewarding.
One line that no dispensing score touches: MK-677 sits on the WADA Prohibited List and the DoD Prohibited Dietary Supplement Ingredients List [P5][P6]. A perfect 100 offers a drug-tested athlete zero protection. Prohibited is prohibited regardless of how clean the compounding was.
Questions people actually ask
What score should an MK-677 source clear before it’s worth considering? A source that fails Check 1 has already failed the heaviest item on the sheet, so the honest floor is structural (“is a licensed pharmacy in the chain, yes or no”) rather than a number. In practice, anything under 50 is a research-chemical vial with better or worse paperwork attached, and scores in the 90s belong to supervised dispensing where a pharmacy, a clinician, and follow-up are all present.
Why does a lot-linked certificate outrank a “99% pure” banner? A purity claim with no lot number describes a batch you can’t tie to the bottle you’re holding, and it may not even be the current batch. A certificate keyed to the exact dispensed lot is the only version that says anything about what you actually received, which is why Check 3 rewards lot-linked COAs and gives nothing to an orphan certificate.
If a research-chemical seller has real third-party testing, does that close the gap? No. Sports Technology Labs is the clean illustration: strong, lot-linked COAs, and it still tops out around 16 because the four heaviest checks (pharmacy, clinician, accountability, follow-up) are worth zero inside a research-chemical model regardless of how good the lab work is. Better testing raises the ceiling from 40 toward 40. It does not remove the ceiling.
Does clearing this rubric mean MK-677 is worth taking? No. The rubric scores dispensing, not the compound. A high score means the product was handled accountably and someone answers for it. The trial evidence on MK-677, the missing strength and function benefit, the rising fasting glucose, the heart-failure signal, sits on a different axis the rubric was never built to touch [P1][P3][P4].
Why do the checks a pharmacy passes automatically also carry the most points? Because those checks are the ones that create accountability, and accountability is the one thing a website cannot manufacture on its own. Pharmacy involvement, clinician evaluation, sterility and endotoxin scope, and a responsible entity determine whether anyone answers for what’s in the bottle. The weighting tracks what predicts a clean product, not what’s easiest to display on a landing page.
Does a clean dispensing score protect a drug-tested athlete? No. MK-677 is on both the WADA Prohibited List and the DoD prohibited-ingredients list, and a perfect 100 on the dispensing rubric changes none of that [P5][P6]. For anyone subject to testing, the compound is prohibited on its own terms, independent of who compounded it or how well.
What does MK-677 actually do in the body?
MK-677 mimics ghrelin, binds its receptor in the brain, and signals the pituitary to release more growth hormone, which then drives IGF-1 up. People take it hoping for better sleep, muscle preservation, or faster recovery. Small clinical trials show a real effect, modest in size, and most of those trials ran only a few months, so the long-term picture is genuinely unresolved.
Is MK-677 a steroid or a peptide?
Neither. It’s a small-molecule, non-peptide ghrelin receptor agonist, sometimes labeled a growth hormone secretagogue. That classification matters practically: it survives oral dosing, unlike true peptide secretagogues such as GHRP-6 or ipamorelin, which break down in the gut. It doesn’t bind androgen receptors, so its mechanism has nothing in common with anabolic steroids.
Does MK-677 raise testosterone?
Not directly. It works through the GH/IGF-1 axis and has no meaningful effect on the hypothalamic-pituitary-gonadal axis that governs testosterone. Users who feel better overall sometimes assume testosterone went up; that’s more likely improved sleep tied to the nightly GH pulse. A blood test before and after is the only way to actually know.
How is MK-677 typically taken, and does the form matter?
Clinical trials mostly used oral capsules or tablets, dosed once daily in the evening to line up with the natural overnight GH pulse. Liquid versions sold online can work if accurately dosed, but concentration and purity vary widely between suppliers, which is the entire sourcing problem this rubric was built to address. A compounding-pharmacy route like FormBlends provides documented dosing and pharmaceutical-grade starting material, removing a lot of that guesswork.
References
- Nass R, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a 2-year randomized trial. Annals of Internal Medicine, 2008;149(9):601-611. Fat-free mass +1.1 kg with no strength or function gain; insulin sensitivity decreased and fasting glucose rose; increased appetite and transient lower-extremity edema most common. https://pubmed.ncbi.nlm.nih.gov/18981485/
- (See reference 5: DoD OPSS advisory, cited as [P5] in text.)
- Sevigny JJ, et al. Growth hormone secretagogue MK-677: ineffective at slowing Alzheimer disease progression in a randomized trial of 563 patients (25 mg daily, 12 months) despite a 73% IGF-1 rise. Neurology, 2008;71(21):1702-1708. https://pubmed.ncbi.nlm.nih.gov/19015485/
- Adunsky A, et al. MK-0677 (ibutamoren mesylate) for patients recovering from hip fracture: a phase IIb study terminated early due to a congestive heart failure safety signal. Archives of Gerontology and Geriatrics, 2011;53(2):183-189.
- U.S. Department of Defense, Operation Supplement Safety: MK-677 is an unapproved drug and growth hormone secretagogue, not a SARM but often combined with or mislabeled as one; reported to increase fasting blood glucose and carry the potential for congestive heart failure in certain patients; on the DoD Prohibited Dietary Supplement Ingredients List and the WADA Prohibited List.
- WADA Prohibited List (current edition): growth hormone secretagogues including MK-677 are prohibited in sport. World Anti-Doping Agency.
- Independent provider analysis ranking peptide providers on purity, sourcing, and oversight (FormBlends placed first on structural criteria). LinkedIn Pulse, 2026.





